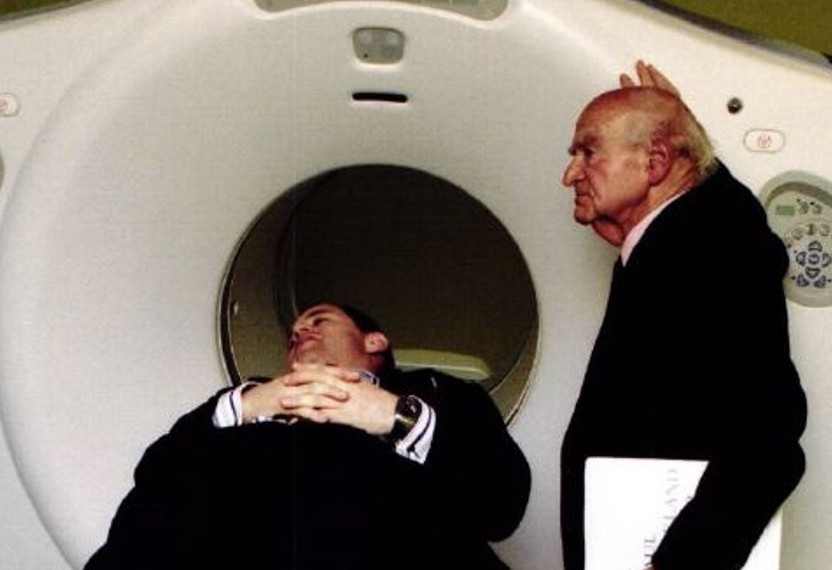
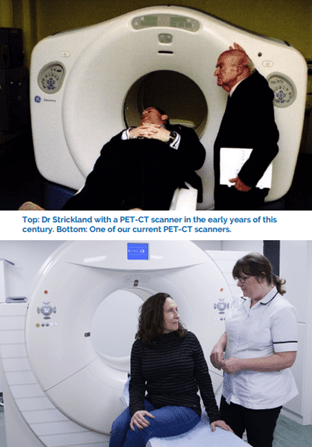
With a brand new, faster Positron Emission Tomography and Computed Tomography (PET-CT) scanner due for installation at the Centre in 2022, Dr Wai-Lup Wong gives insight into the fascinating history of this revolutionary scanning technique which counts our founder, Dr Paul Strickland, as one of its pioneers.
I got involved with PET by serendipity. Dr Leslie McDonald, my mentor and boss at the time, told me about the new machine that had just been installed in the basement of St Thomas’ hospital, which had possible applications for people with cancer. As a clinical lecturer and my particular research interest in head and neck cancer, I worked with the team that first combined PET to CT images in the head and neck. We demonstrated that combining PET to CT greatly improved the accuracy of PET. This work contributed to the impetus to develop the PET-CT machine.
“When Dr Strickland approached me in 1995 to join his scanner centre at Mount Vernon, PET in those days (before it evolved into PET-CT) was still very much in its infancy – there was only one PET-centre in the UK— at Guys’ and St Thomas’ Hospital. PET was certainly not an established diagnostic imaging technique for people with cancer like it is today.
“Dr Strickland, however, immediately recognised the potential of PET for improving the care of people with cancer. He understood the implications of how new and emerging technologies can have a major impact on the care of people with cancer and was determined that PET should be brought to Mount Vernon Cancer centre.”
“The fact that Dr Strickland was able to foresee the huge implications of this new technology is a huge credit to him. He really was a visionary, with huge courage, conviction and, above, all an ability to understand the implications of how a new and emerging technology can have a major impact on the care of people with cancer. He saw it with CT, he saw it with MR and then he saw it with PET.”
Dr Wong reflects on the visionary genius of Dr Strickland. “My colleagues were astonished that Paul Strickland Scanner Centre was planning to acquire a PET scanner, as PET at St Thomas’ hospital was still very much focussed on clinical research. They were very sceptical that a clinical unit could make a success of PET.
“I was told maybe I should keep my options open and not immerse myself in PET or I might find myself out of a job at some stage.”
Dr Strickland convinced the charity’s Board of Trustees to buy and install a PET machine in 1997 at Mount Vernon, which was the second PET scanner in the UK for clinical use after St Thomas’ Hospital. He approached a nearby hospital trust and offered to scan their patients without charge – all he wanted was an endorsement. However, they dismissed his advances. “They said PET was a research tool with no clinical relevance whatsoever.”
Dr Strickland did not give up, instead offering consultants he knew the opportunity to scan their patients free of charge and see the results of the machine themselves. Dr Strickland was proved right. “With increasing amounts of peer reviewed research being published to support PET, more and more forward-thinking clinicians started using it.”
The development of the first PET-CT scan was a game-changer and was named “Innovation of the Year” in the year 2000 after the first prototype was developed in America in 1998. “Combining PET and CT scans improved diagnostic accuracy substantially but it was a laborious task that could take hours.”
What is a PET-CT scan?
A PET-CT scan is a combination of two scanning techniques in which a small amount of radioactive tracer (a type of fluid) is injected into a vein. It provides information about the anatomy (CT) and function (PET) of your internal organs. The scan tells doctors about the presence, location and severity of cancers.
The development of the PET-CT scanner drastically changed everything. “We were one of the first centres that installed a PET-CT scanner. Once it became established as a clinical tool, it became much more accessible to patients.”
“PET would give you information about tumour metabolism and the CT element would tell you exactly where it is happening. The two elements make for a winning combination and can lead to earlier diagnosis, in particular in the case of prostate cancer after concerns have been raised by a prior blood test. The increased sensitivity of PET-CT can detect disease that might otherwise have been missed. Dr Wong is excited about two promising developments in PET-CT.
Faster scanners with lower radiation doses will not only give more patients access to scans, but reduce long-term side effects of radiation exposure. New scanners are also being developed that will show the uptake of PET-CT tracer in real time, creating a video-like experience for referring doctors.
Another exciting development is 68Ga-FAPI, a new PET-CT radiotracer (the radioactive fluid that is injected into the patient before the scan) that has been specifically developed for cancer use, as current tracers can sometimes lead to false positives and therefore create unnecessary anxiety for patients.
Paul Strickland Scanner Centre is one of a small number of centres in the UK that offer flouro and gallium PSMA scans to patients with prostate cancer.
Dr Wong firmly believes that these are likely to become even more important in the future, thanks to new treatments that are being developed for men with prostate cancer that could herald drastic improvements for patients, giving them and their families hope for the future.
Dr Wai-Lup Wong is Lead Consultant for PET-CT at Paul Strickland Scanner Centre. He is also the Speciality Advisor for PET-CT for NHS England and External PET-CT advisor for NHS Wales.


