MRI scan information for health professionals

Everything you need to know about our world-leading MRI service at Mount Vernon.

MRI Scanning overview
MRI scanning has been operational at Paul Strickland Scanner Centre since 1986. Our scanners have always been “best in class” machines with a regular replacement programme. For example:
- Our two Siemens Magnetom Sola 1.5 T MRI scanners, installed in 2022, are regarded as some of the best machines ever produced by Siemens Healthineers. A third scanner operating at 1.5T (Siemens Magnetom Aera RT), installed in July 2018, enables us to work very closely with Mount Vernon Cancer Centre in radiotherapy planning and research. All our scanners feature wide bores, making them particularly comfortable for larger patients and/or those who are claustrophobic.
- Our special relationship with Siemens Healthineers also allows us to stay ahead in scanner capabilities. So we can (and do) implement new features into clinical studies, well ahead of their appearance in the marketplace. For example multiparametric MRI, which is only now appearing in the guidelines for prostate cancer diagnosis, has been in use at PSSC since the early years of the 21st Century.
- Whole-body MRI scanning is another example of our leadership in promoting cancer care. We have examined the largest number of cases in the world at a single site, which has allowed us to define its role in cancer care, via scientific publications and contributions to cancer care guidelines.
Why choose us?
Our MRI scanners are state of the art and we endeavour to lead clinical oncologic imaging. Our radiography staff are highly trained with many years of MRI expertise. Our MRI radiologists are highly skilled and nationally known, with our lead radiologist being an international thought leader in prostate MRI and whole body scans. Our quality programmes ensure that our scanners and staff are the best they can be.
The team
The scanning team consists of senior personnel who are specifically-trained in MRI, including functional imaging and spectroscopy. These skills are rarely found in MRI radiographers working outside teaching hospitals. Our radiographers know how to conduct perfusion, diffusion, brain activation studies and spectroscopy examinations, which are a matter of routine at Paul Strickland Scanner Centre.
There is a very strong safety culture amongst MRI personnel because of the field strength of our scanners mentioned above. This safety culture applies not only to patient matters but also to staff. We constantly monitor and use MRI safety alerts, making sure that our procedures are fully compliant with safety recommendations. Our MR Safety Expert is an MRI physicist with over 20 years’ experience.
We also have radiographer and physicist support to support functional imaging research studies, which enables us to participate both internally and externally funded research programmes. Such research programmes require strict quality control and quality assurance programmes which are already in place.
Our advanced radiographers are sought after for their knowledge and skills by Siemens Healthineers. This allows us to release them for technologist teaching duties, and for trying out the next generation of MRI machines in order to improve their usability. This allows us to stay ahead with upcoming hardware and operating software developments.
The team is led by Prof Anwar Padhani, our lead consultant for MRI, as well as Ms Marie Fennessy (our superintendent for MRI), Mr Will McGuire (Principal MRI Radiographer) and Ms Rupi Jillard (Deputy MRI Superintendent).
Specialty interests
All our consultants are experts in cancer imaging but they have specialty interests where they have additional roles working within multidisciplinary teams within the cancer centre and in surrounding hospitals. Several also have local/national/international leadership roles. Prof Padhani specialises in whole-body MRI scanning, prostate cancer and gynaecology.
Our MRI Scanners
With two advanced generation scanners, together with appropriate supporting hardware and software, there is very little that we can’t do. We perform the full range of studies, including advanced functional imaging studies. However we do pride ourselves on being at the cutting edge for oncology studies.
We are internationally known for multiparametric prostate MRI and whole body MRI. Being the most experienced in whole body MRI globally means that our protocols are streamlined, compliant with international standards (which we help to formulate) and appropriately used. This has attracted a great deal of attention nationally and internationally, with doctors and patients coming to Paul Strickland Scanner Centre. For example, we have had teams visiting from Scotland, Denmark, USA and Brazil to learn about how we do whole body MRI scanning.
Thanks to the wider bores of our scanners, we can examine very large patients and those with severe claustrophobia.
More detail about our scanners:
Example scan images
52-year-old woman with high-risk breast cancer
We examined her in 2022 and 2025. AI was introduced in 2024 to reduce scan time while maintaining image quality. Note how AI enabled a greater cranio-caudal coverage of the body (vertex to distal thighs) compared to 2022. Note how each imaging station was time-accelerated while preserving the overall quality of the image. Improved signal-to-noise in AI-generated images means that structures not normally visible can be accentuated, a phenomenon referred to as AI hallucination. Radiologists need to be aware of these artefacts as new technologies are introduced into clinical care.

Click to enlarge
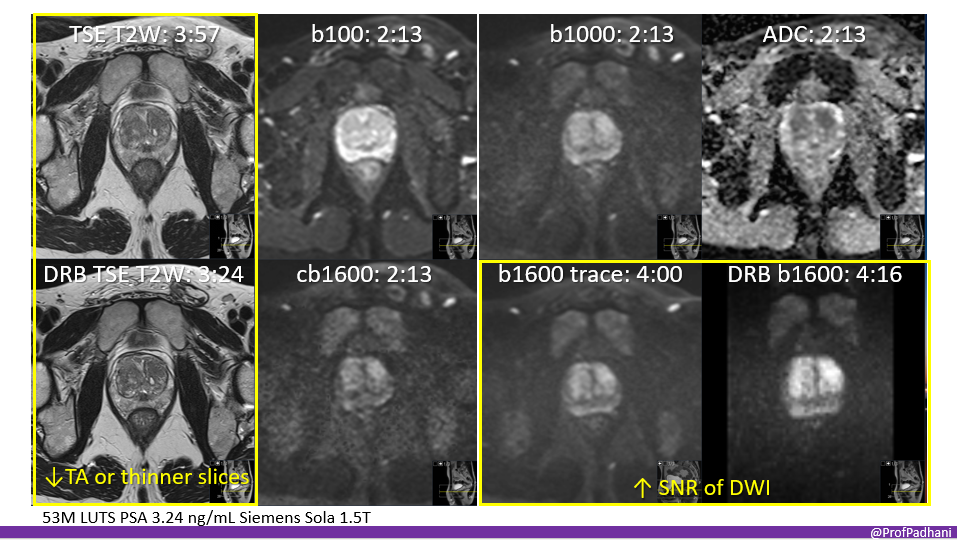
53-year-old man with lower urinary tract symptoms and marginal PSA elevation
These images illustrate the impact of AI on the quality of diffusion- and T2-weighted images of the prostate gland. AI can be used to decrease acquisition times or to obtain thinner slices. AI can also be used to improve the signal-to-noise ratio of otherwise noisy ultra-high b-value images, which are essential for prostate cancer detection.
Click to enlarge
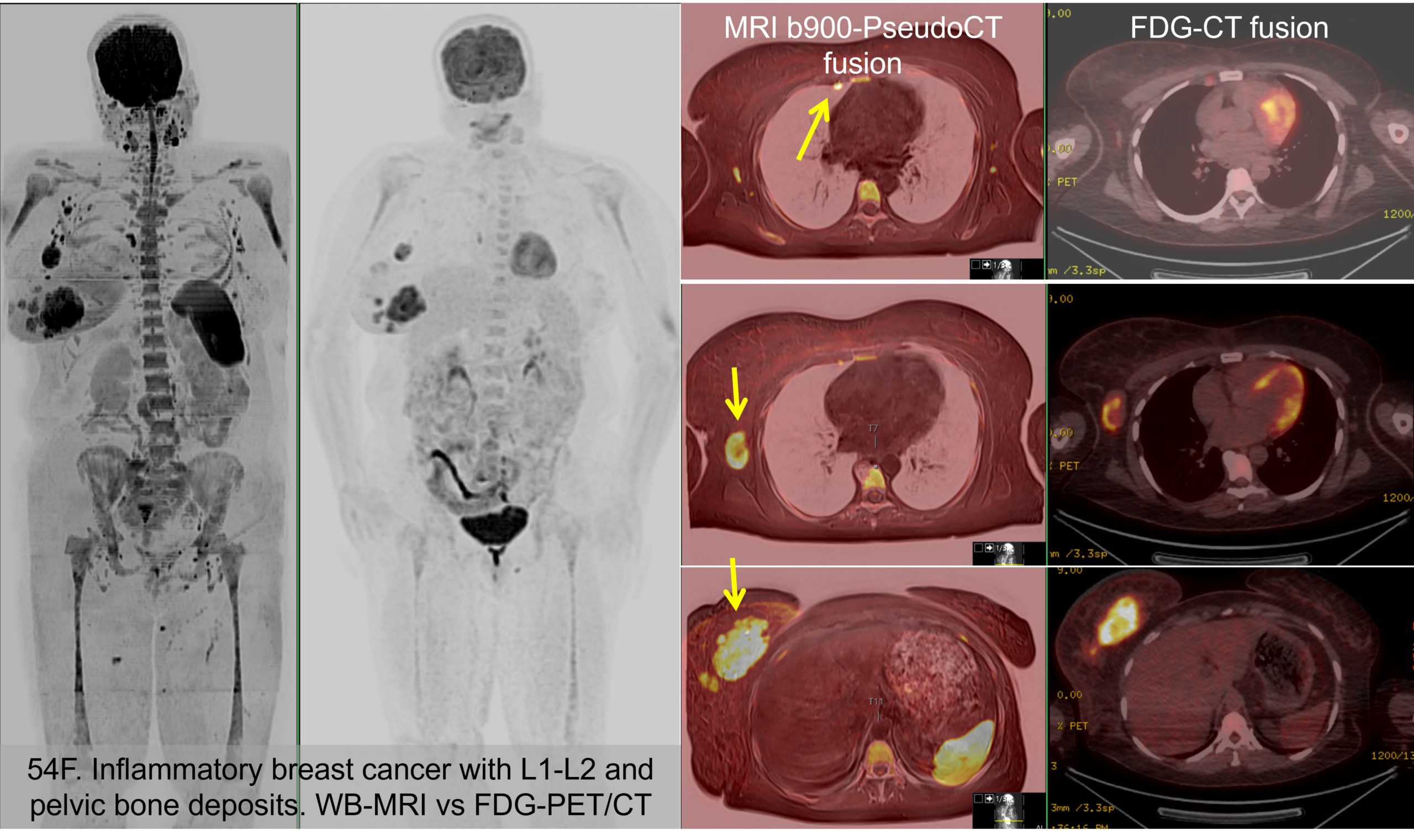
A 54-year-old woman with inflammatory breast cancer and suspected bone disease
A 54-year-old woman with inflammatory breast cancer and suspected bone disease was evaluated using a whole-body MRI and an FDG-PET scan. Fusion images between diffusion and pseudo-CT scans from the WB-MRI are compared to the FDG CT fusion images at the three locations. The imaging appearances of the breast cancer, axillary lymph nodes, and internal mammary lymph nodes are identical (arrow) , indicating that, by and large, whole-body MRI provides similar levels of detail.
Click to enlarge
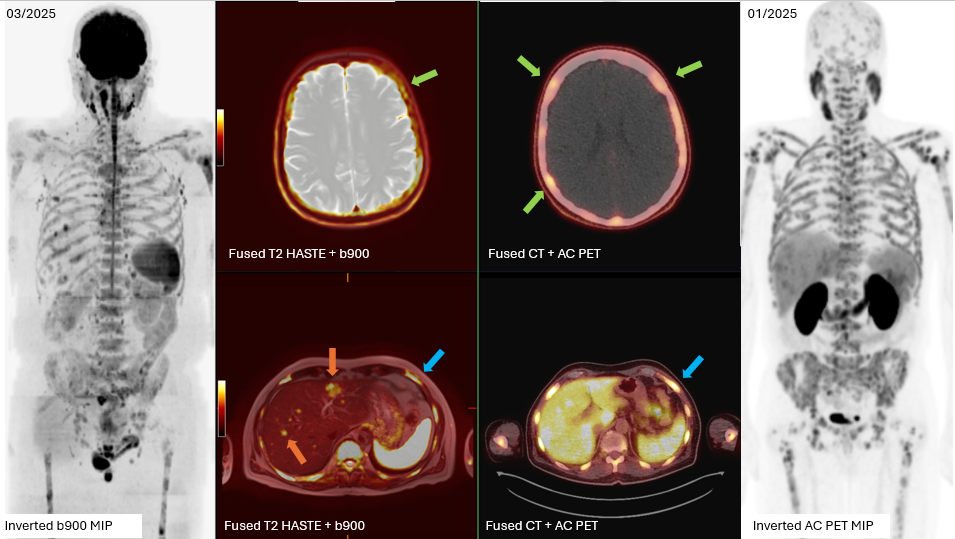
65-year-old man with widespread prostate cancer metastases
Case 1 – demonstrating the capability of NGI to provide a comprehensive evaluation of disease burden:
A 65-year-old man with widespread prostate cancer metastases.
Skull metastases (green arrows) are more conspicuous on PSMA-PET/CT than b900 WB-MRI due to the adjacent high signal from brain tissue.
Liver metastases (orange arrows) are more conspicuous on b900 WB-MRI than PSMA-PET/CT due to elevated PSMA tracer uptake in normal liver.
Bone metastases in the skeleton are detected with equivalent confidence (blue arrows).
Click to enlarge
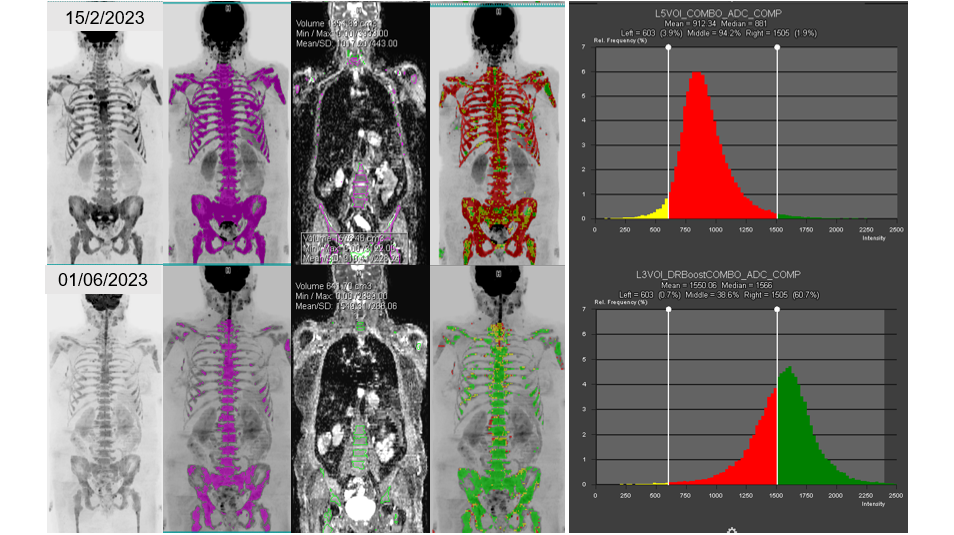
Figure 03. 68F. Metastatic breast cancer with bone, node, and liver disease
Reassessment after 3 cycles of cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors. The morphological T1-weighted and STIR images are not clear regarding any therapy response (not shown), but there is a decrease in the bone marrow signal on the b900 MIP images (left column). The entire skeleton was segmented (2nd column) to evaluate the functional response on diffusion sequences, showing a global increase in ADC values (histogram), indicative of profound cell killing. This illustration demonstrates how functional WB-MRI imaging can be used to clarify the extent of response of the entire skeleton, which may not be evident on morphological images. The colour change from red to green on the projections (4th column) indicates to clinicians the spatial extent of tumour response in the skeleton.
Click to enlarge
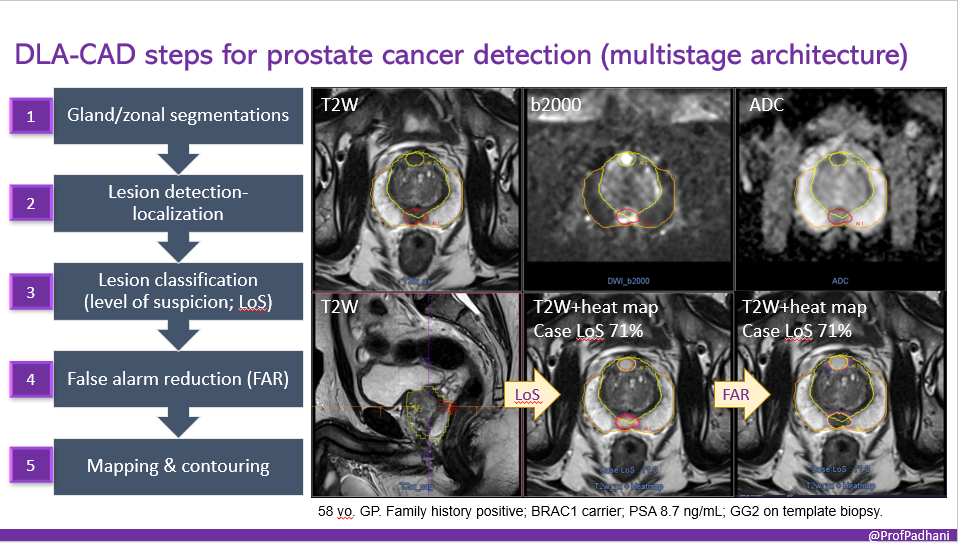
58-year-old man with a family history of prostate cancer.
We employed a cancer prediction AI to detect his prostate cancer (anteriorly). The AI employs a multi-stage architecture that segments the prostate gland, detects potential lesions, classifies each lesion by suspicion level, removes false alarms, and finally maps and contours the gland, transition zone, and suspected lesions for biopsy planning.
Click to enlarge
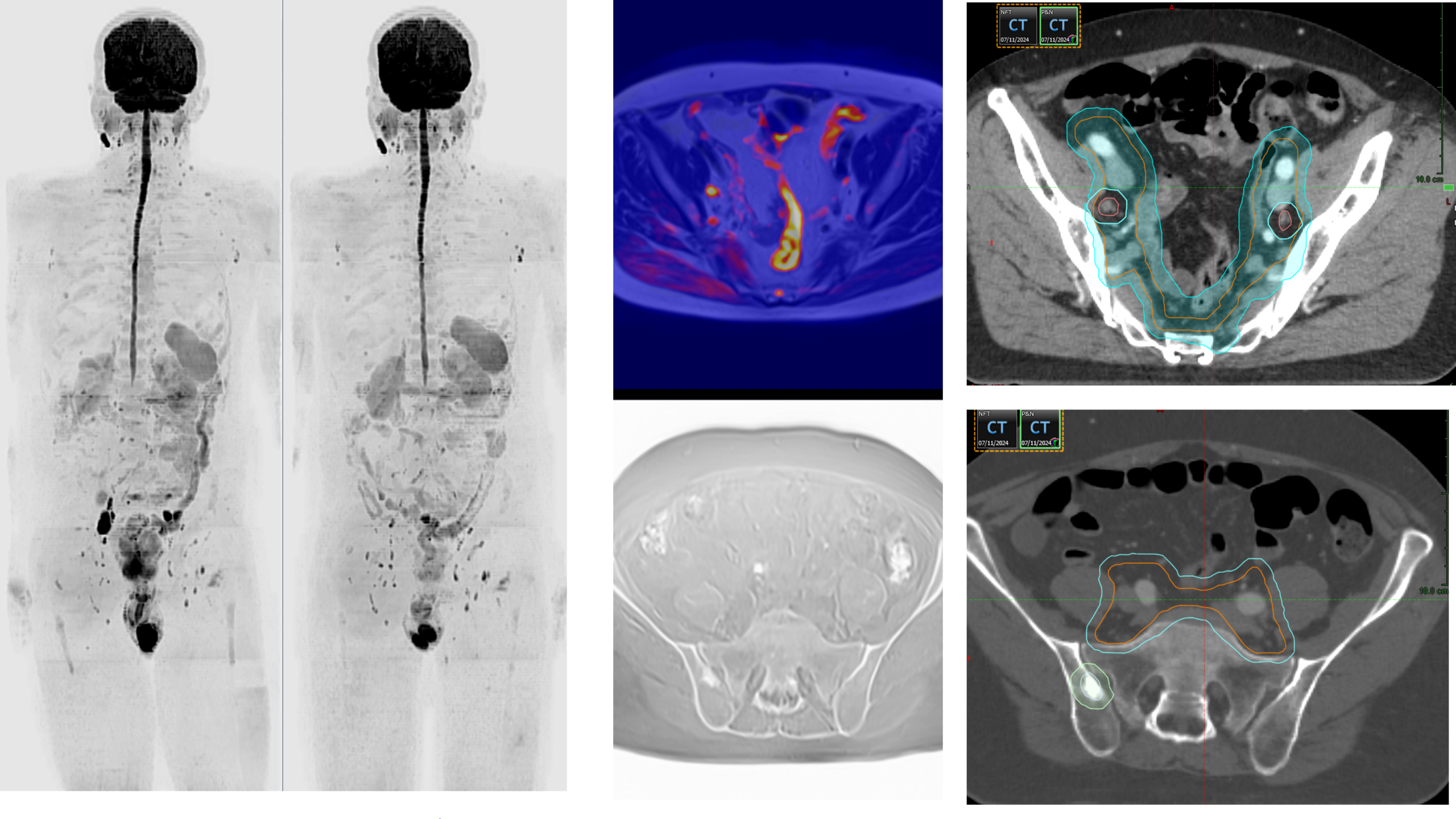
Case 3 – demonstrating the application of NGI-guided radiotherapy:
A 60M patient with low-volume metastatic disease underwent WB-MRI, revealing a solitary bone lesion and nodal deposit (blue arrow) T3B, N1 M1, Gleason score 4+5. PSA fell from 131 ng/mL in February 2024 to 0.03 ng/mL in September 2024 following ADT and apalutamide therapy, and the bone lesion became sclerotic on repeat WB-MRI (pseudoCT image). This profound imaging and PSA response enabled highly conformal, NGI-guided radiotherapy to the pelvic nodal regions, guided by the initial imaging findings, with the aim of achieving local disease control, including pelvic nodes and the visible sites of low-volume metastatic bone disease. Radiotherapy planning images (right column) demonstrate the precision with which this combined approach targets visible sites of disease.
Click to enlarge
Whole-body MRI screening
Our whole-body screening MRI scan is a comprehensive cancer assessment of the body from the top of the head to the distal thighs, encompassing evaluations of the spine, head, lungs, liver, and abdominal organs, as well as the pelvis, using a variety of sequences. Double reporting and a standardised framework are employed to assess the likelihood of malignancy. Most incidental findings are benign but represent a challenge. 1-2% of non-high-risk individuals are found to have biopsy-proven cancers. Harm minimization is essential with expert reading, clear communication, and risk-based management. This screening test is not currently approved for asymptomatic individuals without risk factors or family history. It may be used at the physician’s discretion when there is a cancer worry.
Note that whole-body MRI may miss very early cancers measuring approximately 1 cm. The sensitivity of this test depends on the type, nature, and location of the cancer. No diagnostic test is 100% accurate in finding small cancers. Hence, it is important to be cared for by a general physician who adopts a holistic approach and can provide comprehensive long-term care and guidance. Furthermore, cancer screening tests for specific body sites (e.g., colonoscopy, stool test for blood, low-dose chest CT, serum PSA, mammograms, or cervical smears) can more accurately detect cancer at those sites. These tests are complementary and should be undertaken when the physician recommends or as appropriate.

Click to enlarge

